Practice Essentials
Ebstein anomaly accounts for less than 1% of congenital heart diseases and occurs in 1 in 210,000 live births. The condition occurs with equal frequency in males and females; severely affected neonates can present on the first day of life. Ebstein anomaly may completely escape detection, or patients may not become symptomatic until late in life. In some individuals, Ebstein anomaly is not diagnosed until the eighth decade of life. As many as one half of patients have an atrial septal defect (ASD), and as many as one quarter have an accessory conduction pathway. Newborns may present with functional pulmonary atresia. [1, 2, 3, 4, 5]
(See the images below for Ebstein anomaly in an infant and an adult.)
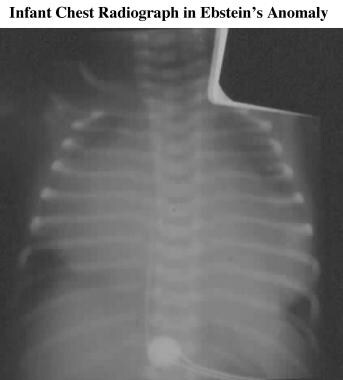 Frontal chest radiograph in an infant with severe Ebstein anomaly shows a large heart with compression of the adjacent lungs. Although the appearance is relatively nonspecific, the large heart should suggest Ebstein anomaly in the differential diagnosis.
Frontal chest radiograph in an infant with severe Ebstein anomaly shows a large heart with compression of the adjacent lungs. Although the appearance is relatively nonspecific, the large heart should suggest Ebstein anomaly in the differential diagnosis.
 Frontal chest radiograph in an adult with Ebstein anomaly shows the abnormal contour associated with distortion of the right ventricle. The pulmonary vasculature is underperfused.
Frontal chest radiograph in an adult with Ebstein anomaly shows the abnormal contour associated with distortion of the right ventricle. The pulmonary vasculature is underperfused.
The tricuspid valve is composed of 3 leaflets, including the anterior, posterior, and septal (also termed mural or medial) leaflets. In Ebstein anomaly, the leaflets are affected to various degrees. The septal leaflet is affected more than the posterior leaflet, which is affected more than the anterior leaflet. [6] The septal and posterior leaflets are often displaced inferiorly toward the apex of the heart.
The anterior tricuspid valve leaflet may be elongated, [7] and it may adhere to the wall of the right ventricle. [6, 8] The septal and posterior leaflets are displaced inferiorly at least 20 mm or 8 mm/m2 in adults. [8, 7] This degree of inferior displacement of the septal leaflet is regarded as definitive. [9, 3]
The leaflets may be tethered by muscular bands or by shortened chordae tendineae and shortened papillary muscles, or the leaflets may adhere directly to the ventricular wall. [6] The valve annulus is not displaced; therefore, it is situated correctly between the atrium and ventricle. Similarly, the proximal attachment of the anterior leaflet to the annulus is normal. [8] The mural leaflet is always present in Ebstein anomaly; if it is absent, the patient's condition is known as unguarded tricuspid orifice rather than as Ebstein anomaly. [10]
Because the annulus is sited anatomically as usual but the septal and posterior valve attachments are displaced inferiorly, a region of the upper right ventricle functionally becomes atrial; this is termed the atrialized portion of the right ventricle. As a result of its structural alteration, this region is thinned and hence prone to aneurysmal dilation, particularly between the attachment of the posterior leaflet and the annulus. [8] Furthermore, the right ventricle has a decreased number of myocardial fibers, which increases the risk of dilation. [10]
Imaging modalities
Traditional imaging modalities for Ebstein anomaly include chest radiography, echocardiography, cardiac catheterization with right ventriculography, and cardiac MRI. [11] Chest radiography is the best initial study, although findings are often nonspecific.
Two-dimensional (2D) echocardiography (seen in the images below) is usually performed next. Echocardiography can help to confirm the diagnosis, assess the severity of the anatomic lesion, and determine the effects on cardiac function. [12, 13, 14, 15, 16] On transthoracic echocardiography, the diagnosis is based on apical displacement of the septal leaflet of the tricuspid valve by 8 mm/m2 or more, along with an elongated sail-like appearance of the anterior leaflet. [17, 4, 18]
 Apical 4-chamber, 2-dimensional echocardiogram in a patient with Ebstein anomaly shows displacement of the tricuspid valve toward the apex of the right ventricle (RV) and tethering of the septal leaflet to the interventricular septum (arrow). LA = left atrium; LV = left ventricle; RA = right atrium.
Apical 4-chamber, 2-dimensional echocardiogram in a patient with Ebstein anomaly shows displacement of the tricuspid valve toward the apex of the right ventricle (RV) and tethering of the septal leaflet to the interventricular septum (arrow). LA = left atrium; LV = left ventricle; RA = right atrium.
 Apical 4-chamber image from 2-dimensional (2D) echocardiography (Echo) in a patient with severe Ebstein anomaly shows displacement of the tricuspid valve towards the apex of the right ventricle (RV) more extreme than that shown in the previous 2 images. The atrialized part of the RV is more dilated and the tethering of the septal leaflet extends further toward the apex here than in Images 10-11. LV = left ventricle; RA = right atrium.
Apical 4-chamber image from 2-dimensional (2D) echocardiography (Echo) in a patient with severe Ebstein anomaly shows displacement of the tricuspid valve towards the apex of the right ventricle (RV) more extreme than that shown in the previous 2 images. The atrialized part of the RV is more dilated and the tethering of the septal leaflet extends further toward the apex here than in Images 10-11. LV = left ventricle; RA = right atrium.
When available and of high quality, cardiac magnetic resonance imaging (MRI) with contrast-enhanced, 3-dimensional (3D) magnetic resonance angiography (MRA) has the potential to replace cardiac catheterization for assessing pulmonary artery anatomy and for providing additional information compared to echocardiography. Some data suggest that MRI and echocardiography should be used as complementary imaging techniques for optimal evaluation before surgery. For example, MRI is preferable when evaluating right ventricular size and ejection fraction and for visualizing the posterior tricuspid valve leaflet, whereas echocardiography may visualize small shunts more readily and may be less likely to underestimate the degree of tricuspid valve regurgitation. [19] MRI can depict anatomy and function with an unrestricted field of view; even the pulmonary arteries and tricuspid valve can be evaluated during a single study. [20, 21]
According to the American College of Cardiology/American Heart Association (ACC/AHA) Guidelines for the Management of Adults with Congenital Heart Disease, [1] determining the anatomy and size of the right atrium and right ventricle in patients with Ebstein anomaly can often be difficult using echocardiography alone, particularly in adults. Cardiac magnetic resonance can provide the information necessary for clinical care and surgical planning because CMR data correlate well with intraoperative findings. In addition, 2D and 3D transesophageal echocardiography can better define the anatomy and function of the tricuspid valve before surgery and provide important information for planning surgical repair.
According to a study by Alsaied et al, right ventricular dysfunction is common after cone operation for Ebstein anomaly and is associated with higher need for postoperative inotropes. Predictors include lower preoperative RV ejection fraction, a more dilated heart, and more severe tricuspid valve abnormality. The authors noted that preoperative cardiac magnetic resonance is an important tool in preoperative assessment and helps predict right ventricular dysfunction. [22]
(A comparison between an MR angiogram and a conventional, contrast-enhanced ventriculogram is shown in the image below.)
 Comparison of conventional contrast-enhanced ventriculogram and 3-dimensional contrast-enhanced magnetic resonance (MR) angiogram. Since MR angiography is performed in 3 dimensions, it can be interrogated with variable image thicknesses to reveal more intracardiac details than that observed with conventional angiography. Conventional contrast-enhanced angiography involves a 2-dimensional acquisition of a projectional image, which cannot be modified in the same way that 3-dimensional MR angiograms can be.
Comparison of conventional contrast-enhanced ventriculogram and 3-dimensional contrast-enhanced magnetic resonance (MR) angiogram. Since MR angiography is performed in 3 dimensions, it can be interrogated with variable image thicknesses to reveal more intracardiac details than that observed with conventional angiography. Conventional contrast-enhanced angiography involves a 2-dimensional acquisition of a projectional image, which cannot be modified in the same way that 3-dimensional MR angiograms can be.
Limitations of techniques
Plain radiographic findings are nonspecific despite occasional pathognomonic appearances. Normal chest radiographic findings do not exclude the diagnosis.
Echocardiography is usually performed after chest radiography; however, if echocardiography is inadequate, MRI can be used to assess anatomy and function. Echocardiography can be limited by poor acoustic windows, especially in patients who are obese, who have undergone surgery, or who cannot lie still. Echocardiography cannot be used to measure the size of the left and right pulmonary arteries. Also note that 2D echocardiographic assessment of the right ventricular size and function may not correlate with the values determined by MRI assessment. [23]
Although MRI is increasingly being performed, potential limitations include availability and expense, the limited availability of qualified personnel to perform the protocol and/or interpret the study, the inability of some patients to cooperate (eg, because of claustrophobia), unsuitability or contraindications (eg, clinically unstable condition, pacemaker, metal objects in an anatomic location where MRI is dangerous and therefore contraindicated), and physicians' unawareness of the uses of MRI.
Pathophysiology
Numerous abnormalities are associated with Ebstein anomaly, including the following:
-
Partial atrioventricular canal [6]
-
Hypoplastic pulmonary arteries [6]
-
Patent ductus arteriosus [6]
-
Parachute mitral valve [6]
-
Cleft anterior leaflet of the mitral valve [6]
-
Left ventricular outflow obstruction [28]
-
Hypertensive pulmonary vascular disease [28]
-
Congenital deaf-mutism [31]
-
Subaortic stenosis [35]
-
Tetralogy of Fallot [36]
Infants with severe Ebstein anomaly and marked cardiomegaly may have further compromise due to excessive bilateral pulmonary compression by the enlarged heart.
Radiography
Classic radiographic features of Ebstein anomaly include a squared-off cardiac contour and pulmonary oligemia (demonstrated in the image below). Cyanosis occurs as a result of a right-to-left shunt, most often at the atrial level, with reduced pulmonary perfusion resulting from ineffective right ventricular ejection.
 The chest radiograph shows classic radiographic features of Ebstein anomaly, including a squared-off cardiac contour and pulmonary oligemia.
The chest radiograph shows classic radiographic features of Ebstein anomaly, including a squared-off cardiac contour and pulmonary oligemia.
Normal chest radiographs with an unremarkable clinical presentation can occur with mild forms of Ebstein anomaly, but this manifestation is not typical.
Cardiomegaly may be seen on chest radiography (as in the first image below). Decreased pulmonary vascularity may be seen in patients with right-to-left shunts, usually through an ASD (see the second image below). A distinctly enlarged right atrium may be identified on chest radiographs. All of these findings can be nonspecific, although in some patients, chest radiographic findings are characteristic.
Frontal chest radiograph in an infant with severe Ebstein anomaly shows a large heart with compression of the adjacent lungs. Although the appearance is relatively nonspecific, the large heart should suggest Ebstein anomaly in the differential diagnosis.
Frontal chest radiograph in an adult with Ebstein anomaly shows the abnormal contour associated with distortion of the right ventricle. The pulmonary vasculature is underperfused.
On the lateral chest radiograph, distortion of the right ventricular outflow tract (see the image below) or displacement by the atrialized segment of the right ventricle may cause abnormal filling of the retrosternal clear space. This finding is of use in older children and adults. The presence of the thymus makes this finding irrelevant for the diagnosis of Ebstein anomaly in infants.
 Lateral chest radiograph in an adult with Ebstein anomaly shows filling of the retrosternal clear space (arrow) related to distortion of the right ventricle.
Lateral chest radiograph in an adult with Ebstein anomaly shows filling of the retrosternal clear space (arrow) related to distortion of the right ventricle.
Computed Tomography
Although Ebstein anomaly can be evaluated by means of computed tomography (CT) scanning, MRI has largely supplanted CT.
On a cardiac CT scan, the right atrium and ventricle appear dilated. A variable degree of apical displacement of the tricuspid valve attachments can be seen relative to the atrioventricular junction. The atrialized and functional portions of the right ventricle may be discerned. The conspicuity of the myocardium may be greater in the functional portion of the right ventricle than in the atrialized portion. Leaflet thickening may be seen. Functional information can be obtained with retrospective gating at the cost of higher radiation dose.
Magnetic Resonance Imaging
When used properly and in suitable patients, MRI can be regarded as the gold standard for detecting Ebstein anomaly and for assessing several aspects of the disease when echocardiography is unable to provide all required information. However, MRI has limitations in evaluating the detail of tricuspid valve morphology, which is best ascertained by using echocardiography. In addition, image quality may be impaired in some patients with arrhythmia.
By using a combination of anatomic (spin-echo sequences and MRA) and functional imaging techniques (cine and velocity encoded), anatomy and function can be assessed reliably by imaging with an area larger than that studied with echocardiography. Even the pulmonary arteries and valve can be evaluated during a single study. [37, 38, 39, 40]
Comprehensive imaging of this type provides a vehicle for surgical planning. The presence of support devices or arrhythmias limits the use of this technique in sick patients.
All 4 types of Ebstein anomaly that Carpentier et al identified and classified can be imaged by using MRI. Young and old patients tolerate MRI well. [41] Critically ill neonates can be imaged in as few as 15 minutes without adverse sequelae. [42] Imaging can be accomplished with 0.5- to 3-T scanners.
Axial spin-echo electrocardiogram (ECG)-gated images are excellent for assessing valvular anatomy, particularly the septal and anterior leaflets (as seen in the images below), right atrial size, and morphology of the atrialized right ventricle. [37]
 Axial ECG-gated spin-echo MRI in a patient with Ebstein anomaly. The patient presented with arrhythmias at the age of 49 years. Image shows enlargement of the right atrium and a dilated right ventricle (RV) compared with the left ventricle. The attachment of the septal leaflet (arrow) of the tricuspid valve is displaced toward the apex of the right ventricle. (Compare this with the level of the mitral valve attachment.)
Axial ECG-gated spin-echo MRI in a patient with Ebstein anomaly. The patient presented with arrhythmias at the age of 49 years. Image shows enlargement of the right atrium and a dilated right ventricle (RV) compared with the left ventricle. The attachment of the septal leaflet (arrow) of the tricuspid valve is displaced toward the apex of the right ventricle. (Compare this with the level of the mitral valve attachment.)
 Axial ECG-gated spin-echo MRI in a patient with Ebstein anomaly shows enlargement of the right atrium (RA). The attachment of the septal leaflet (arrow) of the tricuspid valve is seen displaced toward the apex of the right ventricle (RV). LV = left ventricle.
Axial ECG-gated spin-echo MRI in a patient with Ebstein anomaly shows enlargement of the right atrium (RA). The attachment of the septal leaflet (arrow) of the tricuspid valve is seen displaced toward the apex of the right ventricle (RV). LV = left ventricle.
The posterior leaflet is imaged best in a coronal or oblique-coronal orientation. Coronal and oblique-coronal views can help assess the functional right ventricle. Coronal images can help assess the right atrial size (as in the image below) and conformation of the atrialized right ventricle. [37]
 Coronal magnetic resonance angiogram acquired in an adolescent with severe Ebstein anomaly. Image quality is degraded because of resting tachycardia (heart rate >120 bmp). Image shows a large right atrium (RA), a displaced and distorted right ventricular outflow tract (RVOT), and apical displacement of the tricuspid valve leaflets (between the arrows).
Coronal magnetic resonance angiogram acquired in an adolescent with severe Ebstein anomaly. Image quality is degraded because of resting tachycardia (heart rate >120 bmp). Image shows a large right atrium (RA), a displaced and distorted right ventricular outflow tract (RVOT), and apical displacement of the tricuspid valve leaflets (between the arrows).
Axial images help identify dilation of the tricuspid valve annulus; this identification is achieved by calculating the ratio of the tricuspid ring to the mitral ring (normal ratio = 0.9-1.2). [43]
The degree of tricuspid valve regurgitation or stenosis can be demonstrated by using cine techniques (employed in the image below) and velocity-encoded imaging. [44] In addition, right-to-left shunts through an ASD and right ventricular function can be analyzed using cine and velocity-encoded techniques. [37]
 Axial cine magnetic resonance image in a patient with Ebstein anomaly shows enlargement of the right atrium and right ventricle, along with the loss of signal intensity resulting from tricuspid regurgitation (arrow). The origin (apex) of the area of signal loss, corresponding to the level of coaptation of the valve leaflet, indicates the apical displacement of the tricuspid-valve coaptation.
Axial cine magnetic resonance image in a patient with Ebstein anomaly shows enlargement of the right atrium and right ventricle, along with the loss of signal intensity resulting from tricuspid regurgitation (arrow). The origin (apex) of the area of signal loss, corresponding to the level of coaptation of the valve leaflet, indicates the apical displacement of the tricuspid-valve coaptation.
Cine MRI can demonstrate right ventricular dysfunction and paradoxic motion of the ventricular septum. The abnormal septal motion can, in turn, cause abnormalities of left ventricular morphology and function. [8, 45]
Cine MRI can also reveal the presence of mitral valve prolapse, which is known to result from left ventricular distortion. [6]
Multilevel time-of-flight sequences can be used to demonstrate pulmonary artery anatomy.
Images can be acquired with breath-hold, contrast-enhanced, 3D MRA (used in the image below) rapidly and reliably. Results of a study by Tangcharoen et al showed that MR coronary angiography provides accurate detection of coronary abnormalities, even in patients as young as 4 months. [46]
 Coronal breath-held, contrast-enhanced, 3-dimensional magnetic resonance angiogram (maximum intensity projection) in an adolescent with Ebstein anomaly. The study was performed to assess the size of the pulmonary arteries (arrows) before surgical palliation. Note the huge right atrium (RA), which is seen at the same level as the left ventricle (LV), and the displaced and distorted right ventricular outflow tract (RVOT).
Coronal breath-held, contrast-enhanced, 3-dimensional magnetic resonance angiogram (maximum intensity projection) in an adolescent with Ebstein anomaly. The study was performed to assess the size of the pulmonary arteries (arrows) before surgical palliation. Note the huge right atrium (RA), which is seen at the same level as the left ventricle (LV), and the displaced and distorted right ventricular outflow tract (RVOT).
Baessato et al noted in a study of CMR feature-tracking (CMR-FT) in patients with Ebstein anomaly that CMR-FT was able to describe the complex contractile mechanics of the functional right ventricle. The contractile pattern of the functional RV was characterized by prevalent alterations in the short-axis direction, as indicated by reduced global radial strain (GRS) and global circumferential strain (GCS). CMR-FT uses routinely acquired cine images to assess global and segmental myocardial deformation using 3 strain parameters (longitudinal, radial, and circumferential). [47, 48]
Ultrasonography
Echocardiography is an excellent method for assessing Ebstein anomaly, and it may be the first and only cross-sectional imaging investigation that is required. If inadequate images are obtained, as in evaluating the pulmonary arteries before surgery, or if clinically significant chest deformity is present, MRI or transesophageal echocardiography can be used. Echocardiography can demonstrate elongated tricuspid valve leaflets (especially the anterior leaflet) and leaflet thickening, although the leaflets also may demonstrate a whipping motion. [49, 50, 2, 13, 14, 15]
Prenatal ultrasonography can be helpful in identifying fetal cardiomegaly. Ebstein anomaly with pulmonary atresia has been diagnosed with fetal echocardiography. Hydrops fetalis and Down syndrome have been associated with it. Postnatal echocardiography can be performed in neonates with cyanosis. [51, 52, 53, 54, 55, 56, 57, 58]
The right ventricular cavity is dilated, abnormal septal motion may be observed, excursion of the anterior leaflet may be increased, and leaflet tethering may be seen (as shown in the image below).
Apical 4-chamber, 2-dimensional echocardiogram in a patient with Ebstein anomaly shows displacement of the tricuspid valve toward the apex of the right ventricle (RV) and tethering of the septal leaflet to the interventricular septum (arrow). LA = left atrium; LV = left ventricle; RA = right atrium.
Low-velocity tricuspid regurgitation, which reflects the usual inability to generate high pressure in the right ventricle, is common.
The severity of the lesion can be estimated from the degree of right atrial and ventricular dilation and from marked apical displacement of the tricuspid valve leaflets. The valve can be displaced inferiorly; such displacement is usually to the left. [49]
(See the images below.)
 Short-axis image from a 2-dimensional echocardiogram in a patient with severe Ebstein anomaly shows extensive tethering of the septal leaflet to the interventricular septum. RA = right atrium; LV = left ventricle.
Short-axis image from a 2-dimensional echocardiogram in a patient with severe Ebstein anomaly shows extensive tethering of the septal leaflet to the interventricular septum. RA = right atrium; LV = left ventricle.
 The 2-dimensional echocardiogram shows many of the echocardiographic features of severe Ebstein anomaly: a large right atrium, extensive tethering of the septal leaflet of the tricuspid valve, and a consequently large atrialized segment of the right ventricle. The image demonstrates a large right atrium, which is larger functionally than anatomically because of marked atrialization of the right ventricle; this is a consequence of tethering of the septal tricuspid valve leaflet to the ventricular septum.
The 2-dimensional echocardiogram shows many of the echocardiographic features of severe Ebstein anomaly: a large right atrium, extensive tethering of the septal leaflet of the tricuspid valve, and a consequently large atrialized segment of the right ventricle. The image demonstrates a large right atrium, which is larger functionally than anatomically because of marked atrialization of the right ventricle; this is a consequence of tethering of the septal tricuspid valve leaflet to the ventricular septum.
Wang et al identified extracardiac findings on Doppler ultrasound as independent predictors of perinatal mortality in Ebstein anomaly/tricuspid valve dysplasia (EA/TVD) fetuses, including an abnormal umbilical artery pattern and decreased umbilical vein velocity. [58]
Angiography
Traditional imaging of Ebstein anomaly has included cardiac catheterization with right ventriculography. This method is performed less frequently now, except as part of an ablation procedure for arrhythmias. Relatively noninvasive testing with echocardiography or MRI has reduced the need for diagnostic cardiac catheterization.
Findings are identical to those in MRI and echocardiography, although the images are obtained at increased risk and with a decreased amount of information concerning tricuspid valve anatomy.
(See the image below.)
Comparison of conventional contrast-enhanced ventriculogram and 3-dimensional contrast-enhanced magnetic resonance (MR) angiogram. Since MR angiography is performed in 3 dimensions, it can be interrogated with variable image thicknesses to reveal more intracardiac details than that observed with conventional angiography. Conventional contrast-enhanced angiography involves a 2-dimensional acquisition of a projectional image, which cannot be modified in the same way that 3-dimensional MR angiograms can be.
Contrast angiography demonstrates a large right atrium with a variable degree of tricuspid regurgitation (see the image below). The exact position of the abnormal tricuspid valve may be difficult to determine.
 Right ventricular (RV) angiogram in a patient with Ebstein anomaly shows a dilated RV, opacification of a dilated right atrium (RA) resulting from severe tricuspid regurgitation, and relatively small pulmonary arteries. Contrast material in the right heart chambers obscures detailed information regarding the tricuspid valve anatomy.
Right ventricular (RV) angiogram in a patient with Ebstein anomaly shows a dilated RV, opacification of a dilated right atrium (RA) resulting from severe tricuspid regurgitation, and relatively small pulmonary arteries. Contrast material in the right heart chambers obscures detailed information regarding the tricuspid valve anatomy.
A catheter with a tip electrode (eg, Zukor catheter) can be used to show that atrial pressures are recorded when a right ventricular ECG is detected, indicating displacement of the tricuspid valve toward the cardiac apex.
-
Frontal chest radiograph in an infant with severe Ebstein anomaly shows a large heart with compression of the adjacent lungs. Although the appearance is relatively nonspecific, the large heart should suggest Ebstein anomaly in the differential diagnosis.
-
Frontal chest radiograph in an adult with Ebstein anomaly shows the abnormal contour associated with distortion of the right ventricle. The pulmonary vasculature is underperfused.
-
Lateral chest radiograph in an adult with Ebstein anomaly shows filling of the retrosternal clear space (arrow) related to distortion of the right ventricle.
-
Axial ECG-gated spin-echo MRI in a patient with Ebstein anomaly. The patient presented with arrhythmias at the age of 49 years. Image shows enlargement of the right atrium and a dilated right ventricle (RV) compared with the left ventricle. The attachment of the septal leaflet (arrow) of the tricuspid valve is displaced toward the apex of the right ventricle. (Compare this with the level of the mitral valve attachment.)
-
Axial ECG-gated spin-echo MRI in a patient with Ebstein anomaly shows enlargement of the right atrium (RA). The attachment of the septal leaflet (arrow) of the tricuspid valve is seen displaced toward the apex of the right ventricle (RV). LV = left ventricle.
-
Coronal magnetic resonance angiogram acquired in an adolescent with severe Ebstein anomaly. Image quality is degraded because of resting tachycardia (heart rate >120 bmp). Image shows a large right atrium (RA), a displaced and distorted right ventricular outflow tract (RVOT), and apical displacement of the tricuspid valve leaflets (between the arrows).
-
Axial cine magnetic resonance image in a patient with Ebstein anomaly shows enlargement of the right atrium and right ventricle, along with the loss of signal intensity resulting from tricuspid regurgitation (arrow). The origin (apex) of the area of signal loss, corresponding to the level of coaptation of the valve leaflet, indicates the apical displacement of the tricuspid-valve coaptation.
-
Sagittal-oblique magnetic resonance angiogram in a patient with Ebstein anomaly. A presaturation pulse (dotted line) is positioned through the right atrium to suppress signal from flow originating in that area. A small jet of low signal intensity 0(arrow) indicates a small right-to-left shunt through a patent foramen ovale, which was not visible on color flow Doppler echocardiography (not shown). More than one half of patients with Ebstein anomaly have a right-to-left shunt at the atrial level. The shunts can be large or, as shown here, so small that they are difficult to detect by using conventional techniques.
-
Coronal breath-held, contrast-enhanced, 3-dimensional magnetic resonance angiogram (maximum intensity projection) in an adolescent with Ebstein anomaly. The study was performed to assess the size of the pulmonary arteries (arrows) before surgical palliation. Note the huge right atrium (RA), which is seen at the same level as the left ventricle (LV), and the displaced and distorted right ventricular outflow tract (RVOT).
-
Apical 4-chamber, 2-dimensional echocardiogram in a patient with Ebstein anomaly shows displacement of the tricuspid valve toward the apex of the right ventricle (RV) and tethering of the septal leaflet to the interventricular septum (arrow). LA = left atrium; LV = left ventricle; RA = right atrium.
-
Apical color flow Doppler sonogram in a patient with Ebstein anomaly shows severe tricuspid regurgitation, with color filling the right atrium. Blue = flow away from the transducer; red and orange = aliased high-velocity flow or flow swirling anteriorly around the margins of the right atrium.
-
Apical 4-chamber image from 2-dimensional (2D) echocardiography (Echo) in a patient with severe Ebstein anomaly shows displacement of the tricuspid valve towards the apex of the right ventricle (RV) more extreme than that shown in the previous 2 images. The atrialized part of the RV is more dilated and the tethering of the septal leaflet extends further toward the apex here than in Images 10-11. LV = left ventricle; RA = right atrium.
-
Apical continuous-wave (CW) Doppler image in a patient with Ebstein anomaly. Maximum velocity is only approximately 2 m/s, indicating a systolic pressure difference between the right atrium and the right ventricle of only approximately 16 mm Hg. This result indicates that the right ventricular pressure is not increased; this is the usual circumstance in Ebstein anomaly.
-
Short-axis image from a 2-dimensional echocardiogram in a patient with severe Ebstein anomaly shows extensive tethering of the septal leaflet to the interventricular septum. RA = right atrium; LV = left ventricle.
-
Right ventricular (RV) angiogram in a patient with Ebstein anomaly shows a dilated RV, opacification of a dilated right atrium (RA) resulting from severe tricuspid regurgitation, and relatively small pulmonary arteries. Contrast material in the right heart chambers obscures detailed information regarding the tricuspid valve anatomy.
-
Comparison of conventional contrast-enhanced ventriculogram and 3-dimensional contrast-enhanced magnetic resonance (MR) angiogram. Since MR angiography is performed in 3 dimensions, it can be interrogated with variable image thicknesses to reveal more intracardiac details than that observed with conventional angiography. Conventional contrast-enhanced angiography involves a 2-dimensional acquisition of a projectional image, which cannot be modified in the same way that 3-dimensional MR angiograms can be.
-
The chest radiograph shows classic radiographic features of Ebstein anomaly, including a squared-off cardiac contour and pulmonary oligemia.
-
The 2-dimensional echocardiogram shows many of the echocardiographic features of severe Ebstein anomaly: a large right atrium, extensive tethering of the septal leaflet of the tricuspid valve, and a consequently large atrialized segment of the right ventricle. The image demonstrates a large right atrium, which is larger functionally than anatomically because of marked atrialization of the right ventricle; this is a consequence of tethering of the septal tricuspid valve leaflet to the ventricular septum.







